
 License portability across states has traditionally been the biggest hurdle to a multi-state telemedicine practice. While each state still has its own rules, there are signs that federal site origination rules are lifting and national organizations are seeking new ways to streamline the licensure process. But providers can still run up against a patchwork of payer rules and state laws governing their telehealth practice.
License portability across states has traditionally been the biggest hurdle to a multi-state telemedicine practice. While each state still has its own rules, there are signs that federal site origination rules are lifting and national organizations are seeking new ways to streamline the licensure process. But providers can still run up against a patchwork of payer rules and state laws governing their telehealth practice.
Here is what our experience and research have currently shown true in the telehealth field for clinicians seeking to practice telemedicine across state lines.*
*Full disclosure: The laws are evolving as we write this. Always check with the state licensure board in your region to determine interstate rules for providing patient care. OrthoLive can also help with licensure research.
License Portability
“Decades of evidence-based research highlighting positive patient compliance, clinical outcomes and increasing telemedicine utilization have been met with a mix of strides and stagnation in state-based policy.”
State Telemedicine Gaps Analysis
American Telemedicine Association
Ironically, doctors have been treating their patients across state lines for years, just by talking on the phone to them when they become ill while traveling. The majority of states, however, require physicians to obtain licensing in each state where they sought to practice medicine. This was always generally considered a burden; lengthy and varying application process, examinations, and fees are required by each state licensing board. This piecemeal approach worked well when telehealth was in its infancy. Today, it’s clear that these organizations are struggling to change policies in response to telehealth’s increasing use. A variety of efforts are now underway to change outdated rules in favor of widespread adoption of the technology. One such attempt recently is the Interstate Licensure Compact.
Interstate Licensure Compact
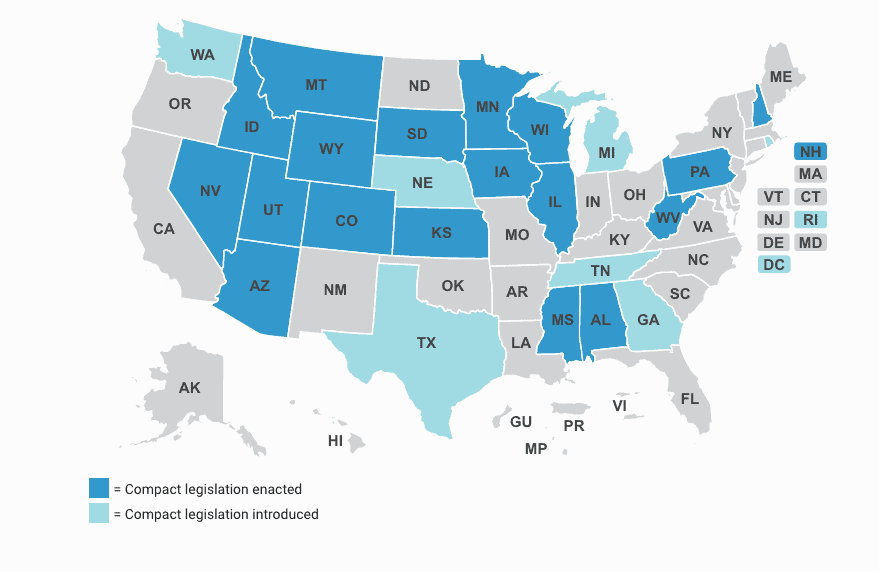
The biggest sign to date that the difficult issue of interstate licensure is slowly being dismantled, is the Interstate Medical Licensure Compact Commission (IMLCC). The organization is now actively processing streamlined state licensure applications across 19 states, opening the door to wider telemedicine applications. It’s the closest national governing body that we have to date to cut through the red tape of patchwork state-by-state clinical licensure rules. (However, this organization is a cooperative and not tied to any federal authority.) Under the organization’s bylaws, participating state medical boards retain their disciplinary authority but share information across state lines.
Currently, there are 20 states fully participating in the compact:
- Alabama
- Arizona
- Colorado
- Kansas
- Idaho
- Illinois
- Iowa
- Maine
- Mississippi
- Montana
- Nebraska
- Nevada
- New Hampshire
- South Dakota
- Tennessee
- Utah
- Washington
- Wisconsin
- West Virginia
- Wyoming
Another dozen states are currently working on passing some formal relationship with the IMLCC. This is phenomenal progress for an organization just a few years old.
Note also that there is a current Nurse Licensure Compact and a Physical Therapy Compact.
Telemedicine Reciprocity Between States?
“In the United States, a tangled web of federal and state regulations controls physician licensing. Although federal standards govern medical training and testing, each state has its own licensing board, and doctors must procure a license for every state in which they practice medicine (with some limited exceptions for physicians from bordering states, for consultations, and during emergencies).”
Health Affairs
Let’s take a real-life scenario an OrthoLive provider recently faced to determine the practical application of telemedicine between states. What are the current rules that apply when a patient lives in Kentucky but their clinical provider is located and only licensed in Tennessee? The answer, at best, is murky, which is why our team is often called upon to share information with providers building their telemedicine practice. In this case, our research determined that licensure is currently required in both states, although there appears to be some “wiggle room.”
First, while Tennessee has signed the interstate licensure, Kentucky has not, although it has introduced this in the state legislature. Next, a closer look at Kentucky state statutes reveals the following language:
A provider must be licensed in Kentucky with the exception of persons who, being nonresidents of Kentucky and lawfully licensed to practice medicine or osteopathy in their states of actual residence, infrequently engage in the practice of medicine or osteopathy within this state, when called to see or attend particular patients in consultation and association with a Kentucky-licensed physician.
The Kentucky Medical Association published a legal handbook last year for physicians practice in the state. There is no mention of telemedicine or interstate licensure. However, the Kentucky Board of Medical Licensure published a Telemedicine Policy Statement in 1997:
Physicians living outside Kentucky but actively practicing medicine upon patients within Kentucky should be required to meet the same statutory qualifications and should be held to the same standards of acceptable and prevailing medical practice within the Commonwealth as are resident physicians practicing within the state.
However, Tennessee statutory rules (§ 63-6-201) state specifically:
No person shall practice medicine within this state unless and until such person has obtained a license from the board created by § 63-6-201.
In 2018, a Kentucky telehealth summit revealed:
- Physicians providing telemedicine are generally held to licensure rules and requirements of the state in which the patient is physically located during the consult.
- The rules differ when the patient is located on a military base.
- There are special rules for the U.S. Veterans Administration.
Attorneys Foley & Lardner suggest that there is a growing list of exceptions to this rule, including:
- A consultation from an out-of-state doctor with a peer licensed in that state may be allowable. (This appears to be true in Kentucky via § 311.560(2)(b)(1).)
- Some states have bordering state rules, allowing out-of-state physicians to cross state lines.
- Special licensure for telemedicine-only care may be allowed.
- Post-operative care via telemedicine may cross state lines.
Perhaps the best document to date to determine the issue comes from a joint document from the Federation of State Medical Boards on their Telemedicine Policies by Board.
- Click here to read the details on Kentucky.
- Click here to read details on Tennessee.
Conclusions
The Milken Institute Review points out, “Pulling back state-level regulation to create a national market has lowered prices and improved services in other industries; it could be expected to do as much for healthcare consumers.”
It is clear that, while the healthcare industry is slowly lifting the barriers to telehealth, they are moving slowly on state licensure. To date, it appears the IMLCC stands the best chance of pushing policy changes at the state level that ease restrictions on multi-state licensure. In the meantime, OrthoLive will continue to help our clients innovate their practices through the use of telehealth. Contact us to find out more.


